Drawing inspiration from the review of design thinking methodology (Figure 8), the final advanced version of a designerly way of doing HPH is the Designerly Way of Conducting HPH (Figure 12), a holistic framework consolidating the crucial elements, mindsets, processes, and methods found in Figures 9-11, effectively unifying them within a single heuristic.
The visual structure of this framework is based on the double diamond design diagram and updated version- framework for innovation. The Double Diamond design diagram is widely used across both design and non-design specialisms. Its popularity stems from its ability to illustrate clearly that the design process is not linear, making it easier for non-design experts to understand designerly thinking. This visual representation has proven effective in communicating the iterative and exploratory nature of the design process, breaking away from the misconception that design follows a linear, top-down approach.
Similarly, this designerly way of conducting HPH visualizes the replicated divergent and convergent processes but not equal space-time frames within a double diamond. Probes, toolkits, and prototypes are methods displayed at different stages: Using probes to better understand and contextualize the social and cultural settings in which HPH projects can be effectively initiated; toolkits can serve as learning materials for HPH organizations, helping them identify beneficiaries’ needs and problems while acting as self-learning materials for HPH beneficiaries, useful during co-creation and for encouraging local engagement; prototypes can function as test experiences and learning tools for beneficiaries, offering a valuable health learning experience.

Table of Contents
- Abstract
- Introduction
- 1. Why Design Thinking for HPH?
- 2. Literature Review
- 3. Results
- 4. Discussion
- Conclusion
- Funding
- Acknowledgements
- Conflicts of Interest
- Author Biographies
- References
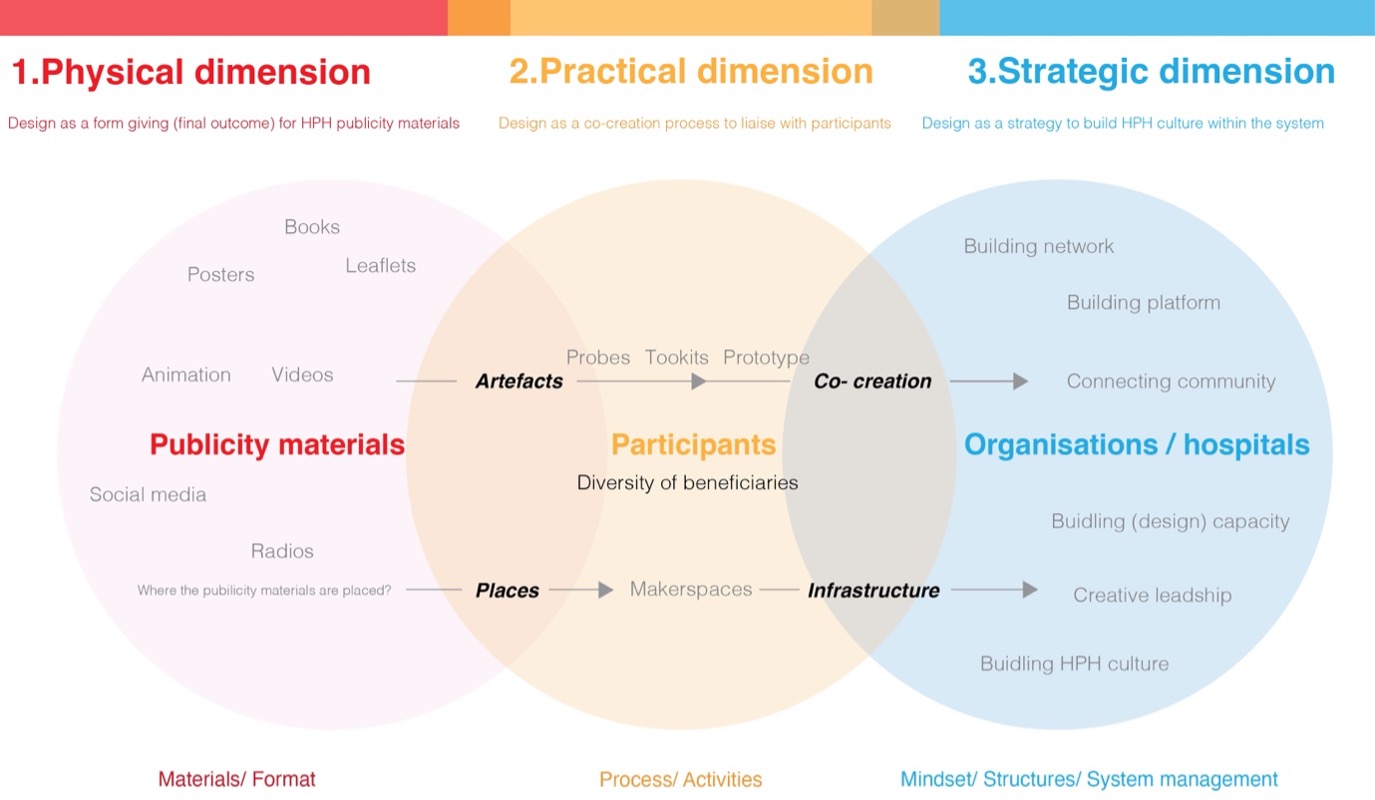
The second space – the practical dimension – proposes that design can function as a co-creation process, an activity involving participants. While publicity materials from the first dimension can be viewed as artifacts, they can also serve as probes, toolkits, and prototypes; key artifacts that can significantly influence the learning experience during co-design activities. Unlike publicity materials, these can be informal and more interactive, adaptive, individualized, diversified and innovative. If Chinese HPH considers suitable locations for promoting publicity materials, the concept of places can be expanded to encompass makerspaces where HPH organizations can host health promoting co-creation and learning activities. This second dimension can be supported by co-design, service design and design ethnography.
The third space – the strategic dimension – considers design as a strategy for establishing an HPH culture within the system. While probes, toolkits, and prototypes from the second dimension can be considered learning materials for co-creation, the concept of co-creation may be further extended to encompass the creation of networks and platforms connecting communities. If the makerspace from the second dimension is infrastructure, it may also contain the development of capacities and HPH culture. These three dimensions operate in parallel rather than hierarchically, maintaining equal importance with different areas of focus. They encompass three distinct dimensions:
- Moving from publicity materials to
- A diverse range of beneficiaries as participants in co-creation activities, finally
- Involving hospitals and HPH organisations to cultivate a sustainable designerly HPH culture.
Nudge theory [35] is employed and transitional communication methods explored in this framework, encouraging a shift in cognitive understanding within Chinese HPH, transitioning from current knowledge to unexplored inquiry through four key transitional conceptual moments: artifacts, co-creation, places, and infrastructure. These interconnect the three dimensions.
Abstract: The delivery of social healthcare services is transitioning from a focus on curative measures to a more proactive approach prioritizing social health promotion. A Health Promoting Hospital (HPH) would ideally evolve beyond the conventional hospital roles of treating illness and managing chronic conditions, encompassing prevention strategies and actively fostering the overall health and wellbeing of patients and community members both within and outside the hospital setting.
In terms of design application within Chinese Health Promoting Hospitals (HPHs), existing studies indicate that hospital management often regards design as a final stage solution rather than embracing a design research perspective that comprehensively and holistically influences the entire process. One approach for all-mass media and graphic design are primary communication approaches for health promotion: marginalized and vulnerable groups are, however, excluded in this approach.
This research proposes three all-encompassing design-thinking frameworks—designerly ways of knowing, thinking, and doing HPH—which serve to enhance the accessibility and inclusivity of design ontology, epistemology, and methodology within the context of Chinese HPH. These design frameworks aid Chinese HPH practitioners in understanding and applying a systematic and holistic view of design thinking for HPH implementation. The ultimate objective is to transform Chinese HPH stakeholders’ understanding of design from a focus on the concrete to the abstract, and from a partial to a more comprehensive perspective within the health promotion context.
This paper provides a showcase on how a comprehensive framework can be constructed through thorough exploration and integration of theoretical and practical aspects across design and non-design domains. It also identifies the three types of design frameworks, offering researchers a valuable resource for understanding the typology of design framework, guiding the development methods of effective design frameworks tailored to research objectives.
Wenbo Ai *
by

2.2. Action Research
2.2.1. Field Trip
The field trip included visiting and interviewing key members staff in charge of health promotion in organisations and hospitals in northern, central and eastern China. The visit covered three healthcare organisations, three rural hospitals, two general hospitals and three specialised hospitals in major cities. The aim was to understand different HPH approaches and design cognitions from central organisation through major hospitals, down to clinics in rural villages. The Design Ladder from the Danish Design Centre [20] acted as an evaluation tool to detect the typologies of design from the HPH practices they had conducted.
Feedback from HPH stakeholders revealed that Chinese health professionals possessed limited understanding of design typologies and their potential value in advancing health promotion. Most stakeholders continued to perceive design as a last-minute intervention, rather than a comprehensive, synthetic design thinking approach rooted in design architecture and research. While stakeholders demonstrated a strong grasp of HPH theory derived from political guidelines, they often struggled to generate innovative ideas when tasked with implementing health promotion projects. Their primary approach tended to revolve around social media and graphic design. This further highlights the pressing need to develop design frameworks within the Chinese context, enabling stakeholders to adopt a designerly approach to HPH implementation.
School of Design, London College of Communication, University of the Arts London, London, UK
* Author to whom correspondence should be addressed.
JDSSI. 2025, 3(3), 26-45; https://doi.org/10.59528/ms.jdssi2025.0825a38
Received: March 19, 2025 | Accepted: July 8, 2025 | Published: August 25, 2025
2.2.2. Case Studies
To establish a theoretical framework—in addition to conducting a thorough literature review and field trips which together generated comprehensive contextual insight—case studies serve as an indispensable method for gaining practical insights into the core subject matter. The researcher conducted two case studies to explore HPH from a design research perspective in his second and third year of the PhD. Case Study (1) focused on enhancing the individual cognitive strategies of low-literate, elderly villagers in managing their medication consumption, considering literacy levels and the significant amount of time spent living independently in the village. The study was conducted in three stages:
- Participatory action research at local hospitals explored how doctors prescribe medicines for low-literate patients.
- Conducting participatory observational interviews with villagers having low literacy levels within the familiar surroundings of their homes. It provided a better understanding of how they store and consume medicines using personal or idiosyncratic methods.
- Based on the first two stages, the researcher organised a participatory workshop to help low-literate villagers design their own methods for memorising medicine dosage and usage.
This approach demonstrated that health promotion could be initiated only after a thorough investigation in both hospital and home environments. This would ensure a rounded understanding of villagers’ contexts: their approaches, needs, and unique challenges related to both health promotion and medical / pharmacological needs.
Case Study (2) conducted a participatory artistic practice to engage children in dental health promotion initiatives. The development stage began with an initial visit to dental hospitals to gain insight into their children's department and dental health promotion methods, then visiting an art school to observe their teaching methods. Subsequently, a co-creation process ensued, involving collaboration between dental professionals from hospitals and teachers from the art school to design a curriculum for learning dental health through art practice. The hospital provided theoretical guidance materials, while art teachers prepared corresponding visual materials for curriculum content development.
Finally, a 12-day course was implemented, involving 12 students aged 4-8, with a researcher and two teaching assistants from the art school delivering the course. The children drew, sketched, made models, bags and dolls, sculpted clay, built 3D structures, role played and learnt different aspects of dental health, such as how to use dental floss, what deciduous or milk teeth are, why bad breath occurs and how to maintain healthy teeth. The course concluded with an interactive exhibition as a means of evaluation. Feedback was gathered using feedback forms and questionnaires designed as games, all of which indicated that the children’s dental care behavior had significantly improved after the course.
Both these two focus groups are considered “extreme users” for whom traditional health promotion methods—leaflets, books, and articles—are often ineffective. These cases demanded the exploration of novel health promotion approaches tailored to the unique needs of each user group. These two case studies contributed to a practical exploration of HPH through a design research pathway and provided practical evidence for developing design frameworks.
Funding
Not applicable.
Acknowledgements
This research study has no funding sources and no potential conflicts of interest. It constitutes a part of the researcher's PhD studies at the Royal College of Art, UK and supported by Professors Teal Triggs and Jo-Anne Bichard. It has involved participants from various groups, including residents from Hantun village, Hujixiang, Shangshuixian, Henan province, children from Timi Art School in Wuhan, China, and gatekeepers and HPH staff from numerous hospitals and health organizations visited during the field trip.
Conflicts of Interest
The author declares that there are no conflicts of interest related to this research.
Author Biographies
▪ Dr. Wenbo Ai is a design researcher, earned his PhD from the Royal College of Art's School of Communication and HHCD Research Centre. He holds a master's degree in service design from the London College of Communication, UAL. Currently, he serves as a Postdoctoral Research Fellow at UAL. Previously, he worked as a Design Research Fellow at the University of Leeds, research assistant at UAL. His research areas are visual communication design, service design, healthcare design, participatory design, design ethnography, user experience, inclusive design, social design, and transition design.
References
1. Wenbo Ai, Integrating design literacy within Chinese health promoting hospitals. PhD diss., London: Royal College of Art. 2023.
2. Rittel, Horst WJ, and Melvin M. Webber. “Dilemmas in a general theory of planning.” Policy sciences 4, no. 2 (1973): 155-169. [CrossRef]
3. Kreuter, Marshall W., Christopher De Rosa, Elizabeth H. Howze, and Grant T. Baldwin. “Understanding wicked problems: a key to advancing environmental health promotion.” Health education & behavior 31, no. 4 (2004): 441-454. [CrossRef]
4. Hunter, D. J. “Getting knowledge on ‘wicked problems’ in health promotion into action.” Health promotion and the policy process (2013): 131-154. [CrossRef]
5. Choi, Edwin, and Juhan Sonin. “Determinants of Health.” GoInvo. n.d. Accessed July 4, 2021. https://www.goinvo.com/vision/determinants-of-health/.
6. Xin, Xiang Yang. “The Thinking Part of Design Thinking.” In Innovation Design Masters’ online lecture. Shanghai: Shanghai Jiao Tong University Press, 2020.
7. Stephan Partelow, “What is a framework? Understanding their purpose, value, development and use.” Journal of Environmental Studies and Sciences 13/3, no. 3(2023): 510-519. [CrossRef]
8. World Health Organization. The Ottawa Charter for Health Promotion. First International Conference on Health Promotion, Ottawa, 1986.
9. Xiong, Mingjie, Liu Xiang, Jia Xiaoyu, and Lian Li. “Review, Comment and Prospect of the Health Promoting Hospital” Modern Preventive Medicine. 44, no. 18 (2017): 3351–3355.
10. World Health Organization. Health Promoting Hospital. WHO, 2025. Accessed July 2, 2025. https://www.who.int/southeastasia/activities/health-promoting-hospital.
11. World Health Organization. Health Promoting Hospital. Geneva: World Health Organization, 2009. Accessed June 23, 2025. https://www.who.int/southeastasia/activities/health-promoting-hospital.
12. World Health Organization. Health Promoting Hospital. Geneva: World Health Organization, 2009. Accessed June 23, 2025. https://www.who.int/southeastasia/activities/health-promoting-hospital.
13. Crosby, Richard, and Seth M. Noar. “What Is a Planning Model? An Introduction to PRECEDE‐PROCEED.” Journal of Public Health Dentistry 71 (2011): S7–S15. [CrossRef]
14. Glasgow, Russell E., Thomas M. Vogt, and Shawn M. Boles. “Evaluating the Public Health Impact of Health Promotion Interventions: The RE-AIM Framework.” American Journal of Public Health 89, no. 9 (1999): 1322–27. [CrossRef]
15. World Health Organization. Ninth Global Conference on Health Promotion: Promoting Health in the Sustainable Development Goals – Health for All and All for Health. Shanghai, China, November 21–24, 2016. Geneva: World Health Organization. Accessed July 4, 2018. https://www.who.int/teams/health-promotion/enhanced-wellbeing/ninth-global-conference.
16. World Health Organization. Promoting Health in the SDGs: Report on the 9th Global Conference for Health Promotion, Shanghai, China, 21–24 November 2016: All for Health, Health for All. Geneva: World Health Organization, 2017. Accessed July 4, 2018. https://www.who.int/publications/i/item/WHO-NMH-PND-17.5.
17. Central Committee of the Communist Party of China and State Council of the People’s Republic of China. Outline of the Healthy China 2030 Planning. Beijing: Central Committee of the Communist Party of China and State Council, issued October 25, 2016. Accessed February 23, 2018. https://faolex.fao.org/docs/pdf/chn175038.pdf.
18. Xiong, Mingjie, Liu Xiang, Jia Xiaoyu, and Lian Li. “Review, Comment and Prospect of the Health Promoting Hospital.” Modern Preventive Medicine 44, no. 18 (2017): 3351–3355.
19. Tian, Xiangyang. A study on Strategies and Models of Health Education and Promotion in Chinese Rural Villages/中国农村健康教育与健康促进策略与模式研究. PhD diss., Fudan University, 2013.
20. Danish Design Centre. “The Danish Design Ladder.” Mr Matt Davies Blog, October –, 2020. Accessed November 4, 2020. https://www.mrmattdavies.me/post/the-danish-design-ladder.
21. Schon, Donald. The Reflective Practitioner: How Professionals Think in Action. London: Temple Smith, 1983.
22. Owen, Charles L. “Design Research: Building the Knowledge Base.” Design Studies 19, no. 1 (1998): 9–20. [CrossRef]
23. World Health Organization. The Ottawa Charter for Health Promotion. First International Conference on Health Promotion, Ottawa, November 21, 1986. Geneva: World Health Organization, 1986.
24. Buchanan, Richard. “Wicked Problems in Design Thinking.” Design Issues 8, no. 2 (1992): 5–21. [CrossRef]
25. Brown, Tim. “Design Thinking.” Harvard Business Review 86, no. 6 (2008): 84–92.
26. Danish Design Centre. “The Danish Design Ladder.” Mr Matt Davies Blog, October –, 2020. Accessed November 4, 2020. https://www.mrmattdavies.me/post/the-danish-design-ladder.
27. Malmberg, Lisa. Building Design Capability in the Public Sector: Expanding the Horizons of Development. Vol. 1831. Linköping: Linköping University Electronic Press, 2017. [CrossRef]
28. Ulloa, Manuela Aguirre. “TRANSFORMING PUBLIC ORGANIZATIONS INTO CO-DESIGNING CULTURES.” 2020.
29. Kimbell, Lucy. The Service Innovation Handbook: Action-Oriented Creative Thinking Toolkit for Service Organizations. Amsterdam: BIS Publishers, 2014.
30. Täuscher, Karl, and Nizar Abdelkafi. “Visual Tools for Business Model Innovation: Recommendations from a Cognitive Perspective.” Creativity and Innovation Management 26, no. 2 (2017): 160–174. [CrossRef]
31. Noble, Ian, and Russell Bestley. Visual Research: An Introduction to Research Methods in Graphic Design. London: Fairchild Books, 2016. [CrossRef]
32. Brown, Tim. “Design Thinking.” Harvard Business Review 86, no. 6 (2008): 84–92.
33. Plattner, Hasso. An Introduction to Design Thinking. Stanford, CA: Institute of Design at Stanford, 2013.
34. Design Council. The Double Diamond. Accessed July 4, 2019. https://www.designcouncil.org.uk/our-resources/the-double-diamond/.
35. Thaler, Richard H., and Cass R. Sunstein. Nudge: Improving decisions about health, wealth, and happiness. Penguin, 2009.
36. Simon, Herbert A. “The Science of Design: Creating the Artificial.” Design Issues (1988): 67–82. [CrossRef]
37. Glasgow, Russell E., Thomas M. Vogt, and Shawn M. Boles. “Evaluating the Public Health Impact of Health Promotion Interventions: The RE-AIM Framework.” American Journal of Public Health 89, no. 9 (1999): 1322–1327. [CrossRef]
38. Roberts, Jess P., Thomas R. Fisher, Matthew J. Trowbridge, and Christine Bent. “A Design Thinking Framework for Healthcare Management and Innovation.” Healthcare 4, no. 1 (2016): 11–14. [CrossRef]
39. Ku, Bon, and Ellen Lupton. Health Design Thinking: Creating Products and Services for Better Health. Boston: MIT Press, 2022. [CrossRef]
Share and Cite
Chicago/Turabian Style
Wenbo Ai, "Design Thinking Frameworks for Sustainable and Inclusive Health Promotion Strategies in China." JDSSI 3, no.3 (2025): 26-45.
AMA Style
Ai WB. Design Thinking Frameworks for Sustainable and Inclusive Health Promotion Strategies in China. JDSSI. 2025; 3(3): 26-45.
© 2025 by the authors. Published by Michelangelo-scholar Publishing Ltd.
This article is published under the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International (CC BY-NC-ND, version 4.0) license (https://creativecommons.org/licenses/by-nc-nd/4.0/), which permits non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited and not modified in any way.
3. Results
Three types of design frameworks were developed at the fifth year of the researcher’s PhD: the designerly ways of knowing, thinking and doing HPH.
3.1. The First Design Framework: A Designerly Way of Knowing of HPH
Based on design thinking epistemology (Figure 6), the first HPH framework (Figure 9) is developed and offers a comprehensive understanding of what design is for HPH and what design can offer to HPH through three spaces. The first, the physical dimension, describes design as material and format, analogous with current Chinese HPH’s understanding and approach to design. This includes traditional media promoting health knowledge through posters, books, leaflets, and videos: printed materials through to social media platforms and mass media channels such as TV and radio. Hospitals typically perceive graphic design and media design as the final dissemination stage of HPH, hiring designers as an “add-on” at this stage.
Design Thinking Frameworks for Sustainable and Inclusive Health Promotion Strategies in China
Introduction
This study was conducted by the researcher as a component of his PhD research (2017-2023), entitled “Integrating Design Literacy Within Chinese Health Promoting Hospitals [1].” The primary research question addressed in the PhD study was, “Can design thinking create a supportive, sustained, and creative community setting for the development, consideration, and implementation of Chinese HPH?” The original PhD addressed a gap in the design of Chinese healthcare research: there was a lack of comprehensive design-based theoretical frameworks—particularly in health promotion—to guide hospitals and healthcare organizations in their practices.
The generation of the design-thinking framework trinity—“designedly ways of knowing, thinking, and doing HPH”—to fill the practical and theoretical gaps guides this paper’s description of HPH design frameworks, a field trip and action research case studies. These design frameworks serve to guide epistemology, research processes, mindsets, methods, and principles specifically for healthcare promotion leaders who are unfamiliar with design research and literacy.
1. Why Design Thinking for HPH?
Health promotion is an ill-defined, wicked problem [2, 3, 4]. The determinants of health diagram from GOIVO [5] illustrates how cultural, geographical, social, ethical, age, education, and genetic-familial influences affect the social determinants of health through multiple factors.
As a result, the design framework should be adaptive and interpretive, following Xin’s concept of design thinking, “a reflective and adaptive approach to problem solving in contexts that are open to interpretation, for goals that are open to negotiation, and with principles that are open to selection [6].”
A framework is, for this context, a synergistic blend of categories, theories, structures, components, or tools derived from initial research, guiding users from theory to practice [7]. Compared to traditional social science research text-based frameworks, a design framework offers a more visually communicative structure that presents information effectively, precisely and practically for the purpose, providing solutions from a design theoretical perspective. Excellent design frameworks can improve capacity, implement comprehensive theory, offer alternative approaches to inquiry as well as vital solutions for wicked problems.
If principals and managers as well as healthcare professionals more widely can understand the nature of design and be encouraged to nurture design capability, a more pluralistic, situated, nuanced and inclusive process for health promotion can be grown within their systems, novel health promotion methods can be designed as well as tools and artefacts for disadvantaged groups.
2.3. Reflections on Case Studies
Following the two case studies, reflection-on-action [21] as a method facilitated the extraction of tacit phenomena, transforming them into explicit knowledge in the fourth year of researcher’s PhD. This allowed for the transition from specific case-based understanding to generalizable knowledge, encapsulating the process of moving from “knowledge building” to “knowledge using;” from an “inquiry paradigm” to an “application paradigm [22].” These shifts in perspective are pivotal in the development of effective frameworks.
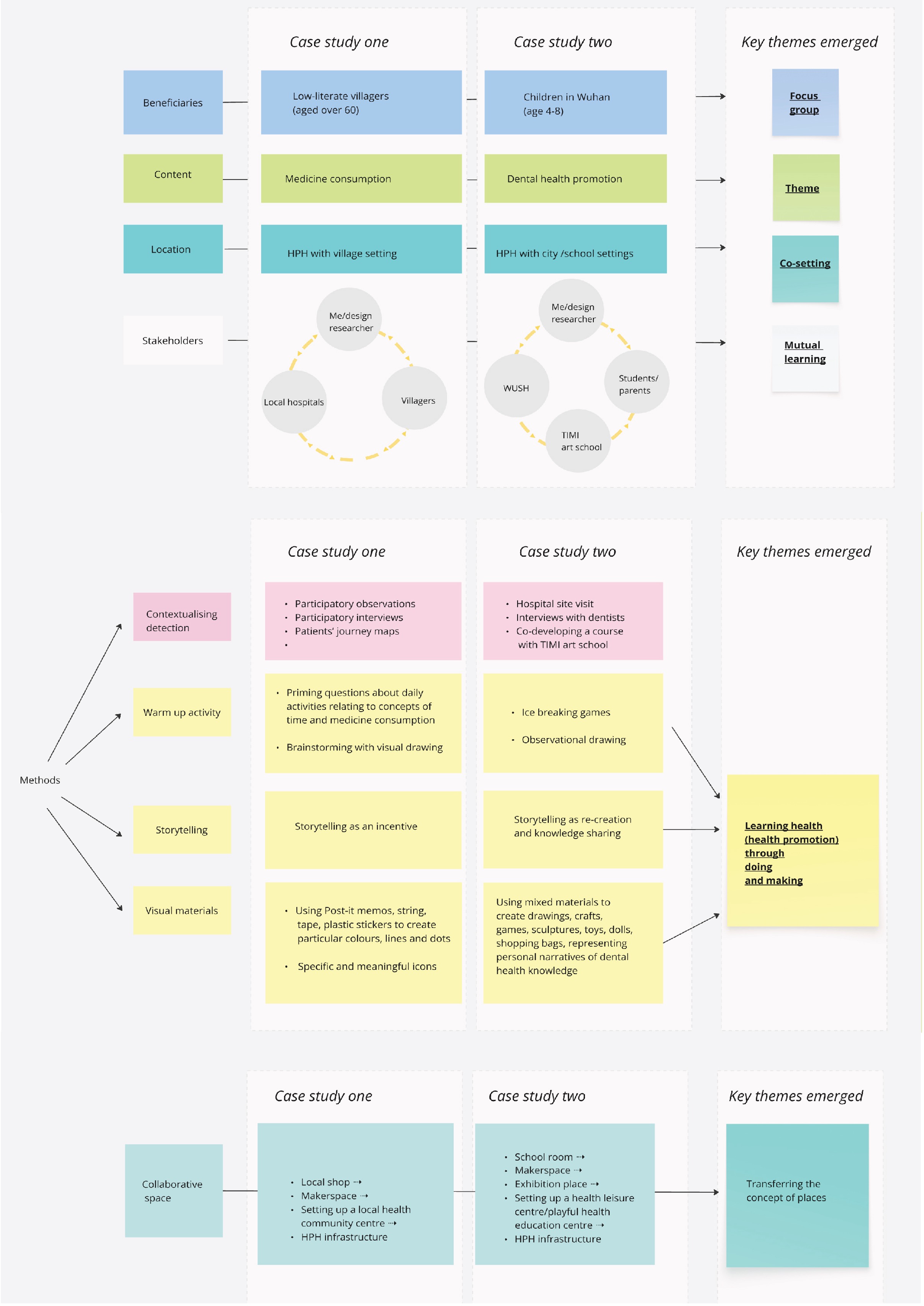
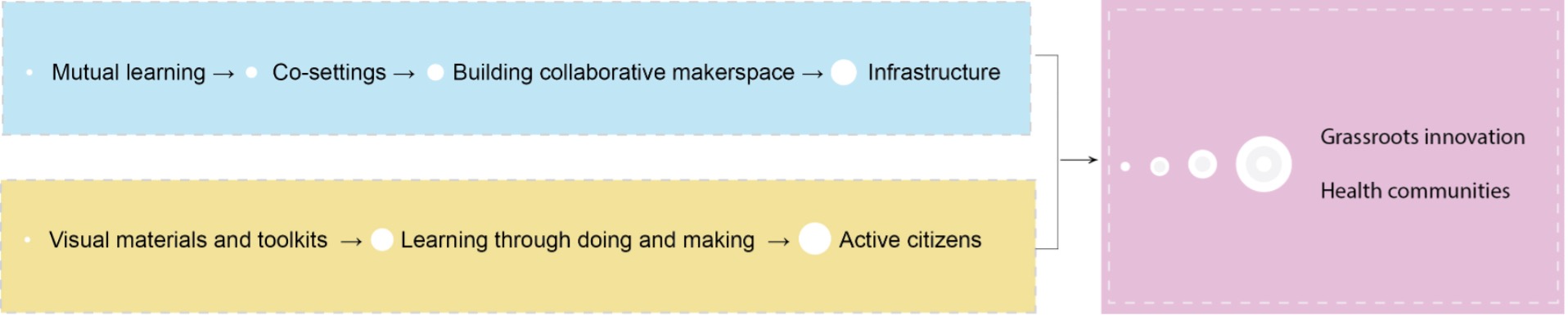
Figure 1 details the specific methods employed, and through a comparative reflection on the case studies, four thematic variables emerged: focus groups, co-settings, mutual learning, and visual materials which enhance learning experiences. Figure 2 demonstrates how these key thematic variables act as transitional threads from micro elements to macro infrastructure. Mutual learning between HPH organisations and focus groups encourages organisations to identify the specific health promotion needs of the focus groups. This is then followed by the creation of collaborative settings and makerspaces. It is here that focus groups can learn through hands-on activities using the visual materials and toolkits developed by HPH organisations based on findings from the mutual learning process. The makerspace may be a temporary public area for hosting health activities in partnership with external collaborators, but it can also serve as a permanent health centre where local residents engage in health education: leisure activities, health exhibitions, games, workshops, reading clubs and lectures. Combining traditional passive learning methods through text and media with such active learning through group-based hands-on activities, aims to promote active, healthy citizens, eventually establishing health community initiatives which allow communities to manage their own health.
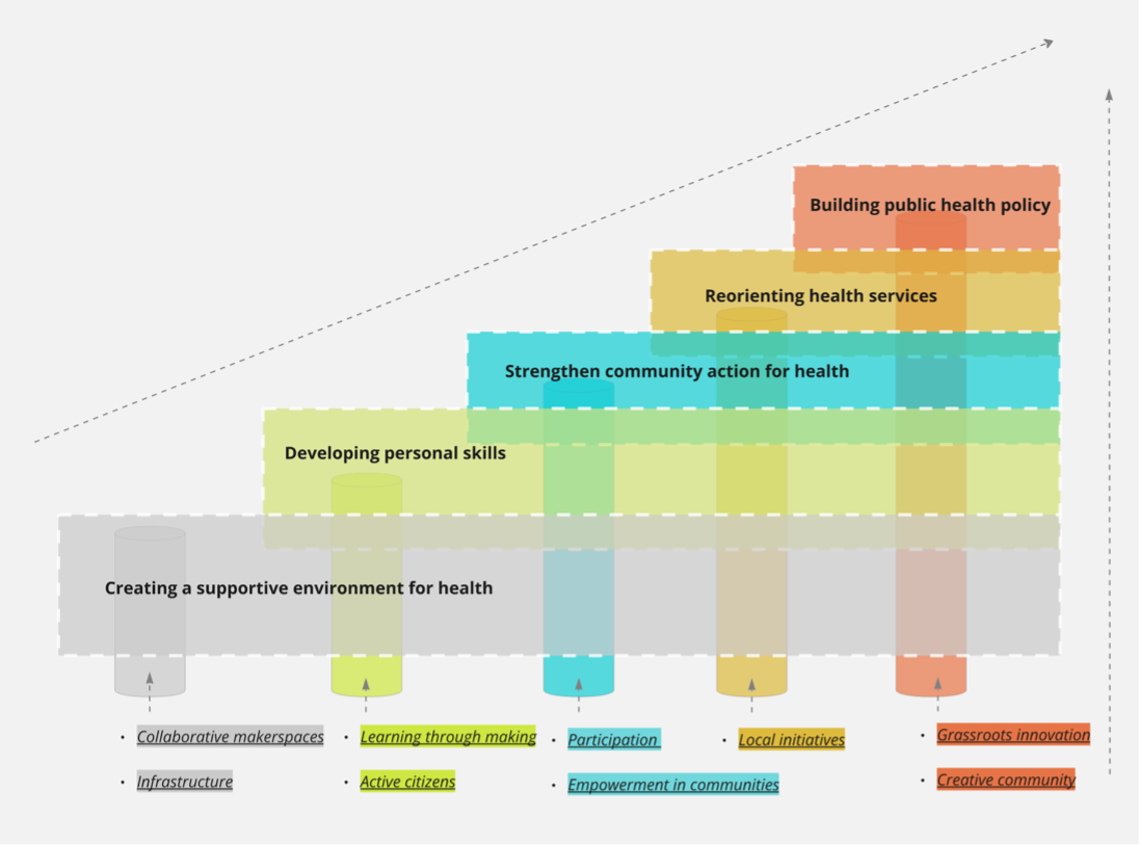

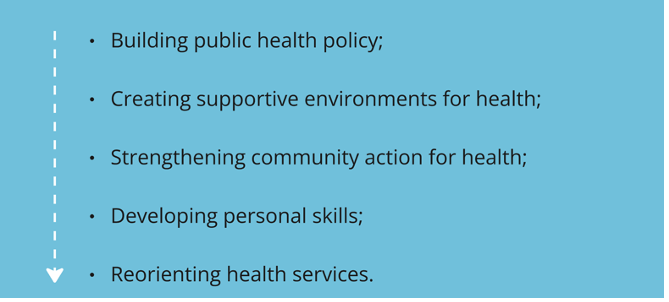
This transitional process offers a bottom-up strategy, distinct from the top-down iterations of WHO’s five actions [23] (Figure 3). The researcher reorganized these five actions using design scaffolding (Figure 4) based on the key themes that emerged from his reflections on theory and practice (Figure 1 and Figure 2). This new approach begins with establishing a supportive environment for health through collaborative makerspaces and building infrastructure. Within this setting, the next step is developing personal skills by fostering active citizenship and promoting learning through practical, hands-on activities. Participation, engagement, and empowerment can strengthen community-driven health initiatives and lead to a reorientation of health services. Ideally, these processes will ultimately contribute to the reformulation of public health policies through grassroots innovation and the creation of engaged communities.
2.4. Design Thinking Frameworks Review
To develop an all-encompassing design framework for HPH, the researcher conducted a thorough examination of existing design thinking frameworks. This review provided a structured foundation and delineated the necessary scope for the ultimate design framework tailored to HPH. Through a review of design thinking frameworks, the overall typology of design thinking can be divided into three categories: design thinking epistemology (Figure 6), design thinking process (Figure 7), and design thinking methodology (Figure 8).
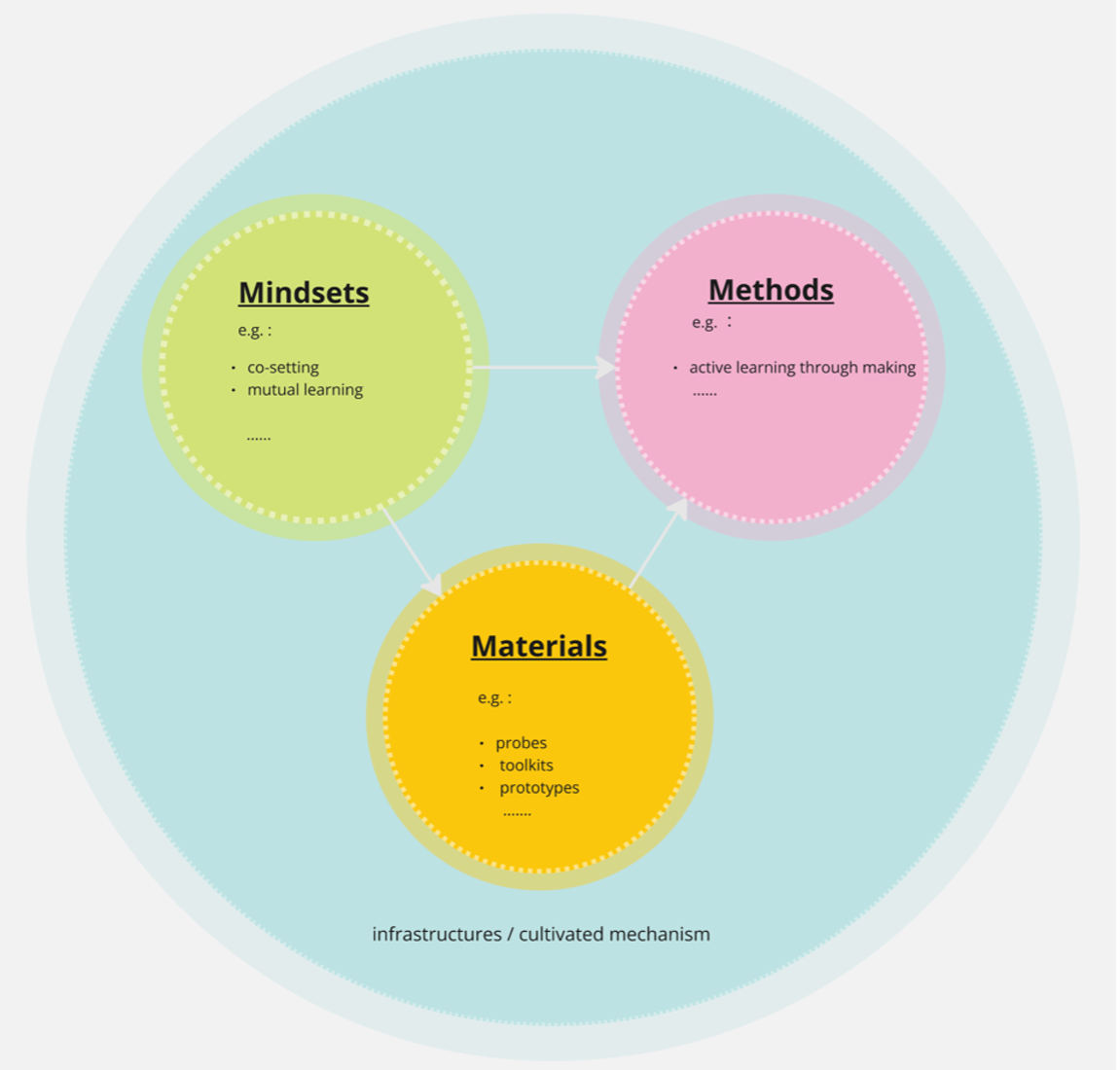
Figure 5 describes three main typologies: mindsets, methods and materials which may cultivate health service mechanisms and HPH infrastructure. Figures 1-5 emerged from a generalization process rooted in reflection-on-action: this self-reflexive process serves as an inevitable means for leaping from action to knowledge and establishing a design framework. These figures and the reflexive processes they map facilitate the transition of tacit phenomena identified through a primary literature review, field trips, and case studies into explicit knowledge, ultimately contributing to the development of design frameworks.
Figure 6 selected 5 types of design thinking epistemology: Four areas of design from Buchanan [24], design thinking from Brown [25], the Design ladder [26], and two design models from doctoral research- awareness of design [27], the Ripple Model [28]. The review of these frameworks offers a foundational understanding of how design thinking can be comprehended and segmented, revealing the epistemology of design thinking.
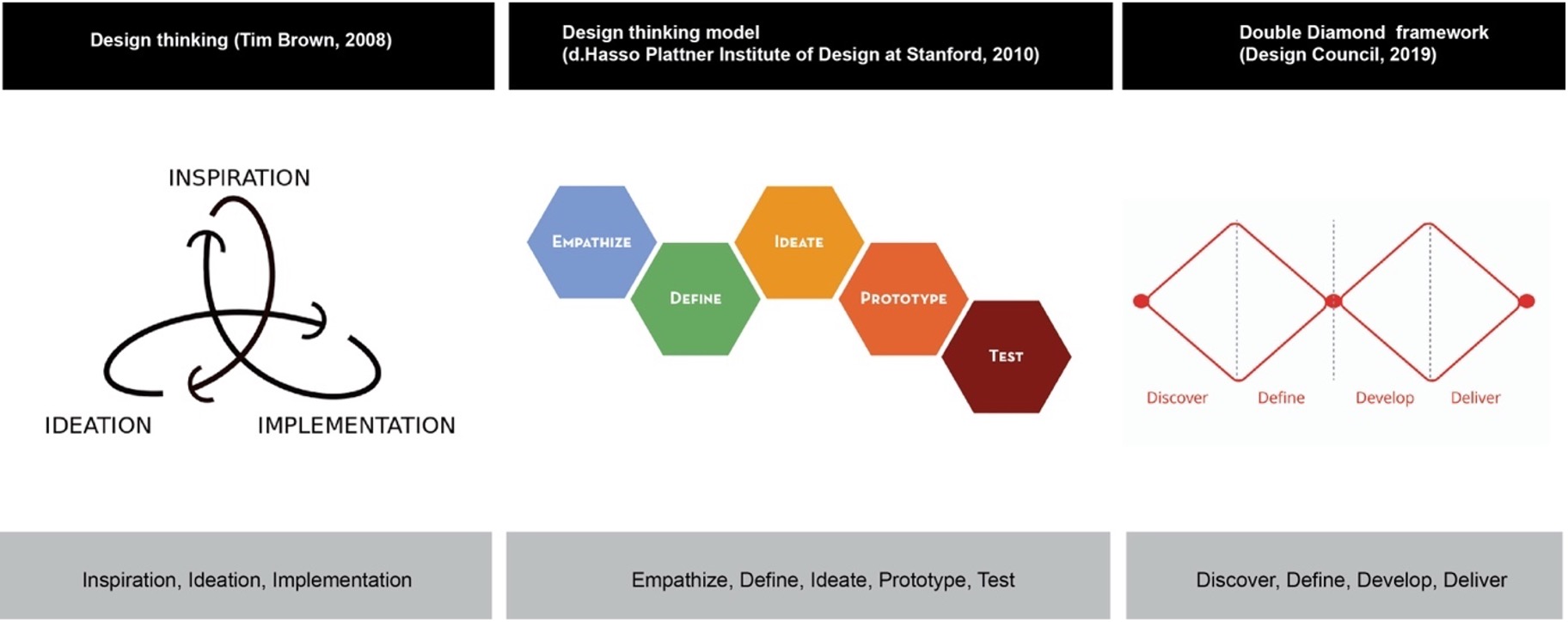
Once we understand what design thinking is, the next stage is to explore how the process works. Given the complexity and abstract nature of design processes, particularly for non-design experts, visual diagrams prove to be valuable tools in illustrating these processes [29, 30], hereby facilitating effective communication of design thinking principles to a diverse audience [31]. The three models depicted in Figure 7 each provide a unique visualization of design thinking processes: “Inspiration, ideation, implementation” from Brown [32]; “Empathize, define, ideate, prototype, test” from Plattner [33], and “Discover, define, develop, deliver” from the UK Design Council [34].
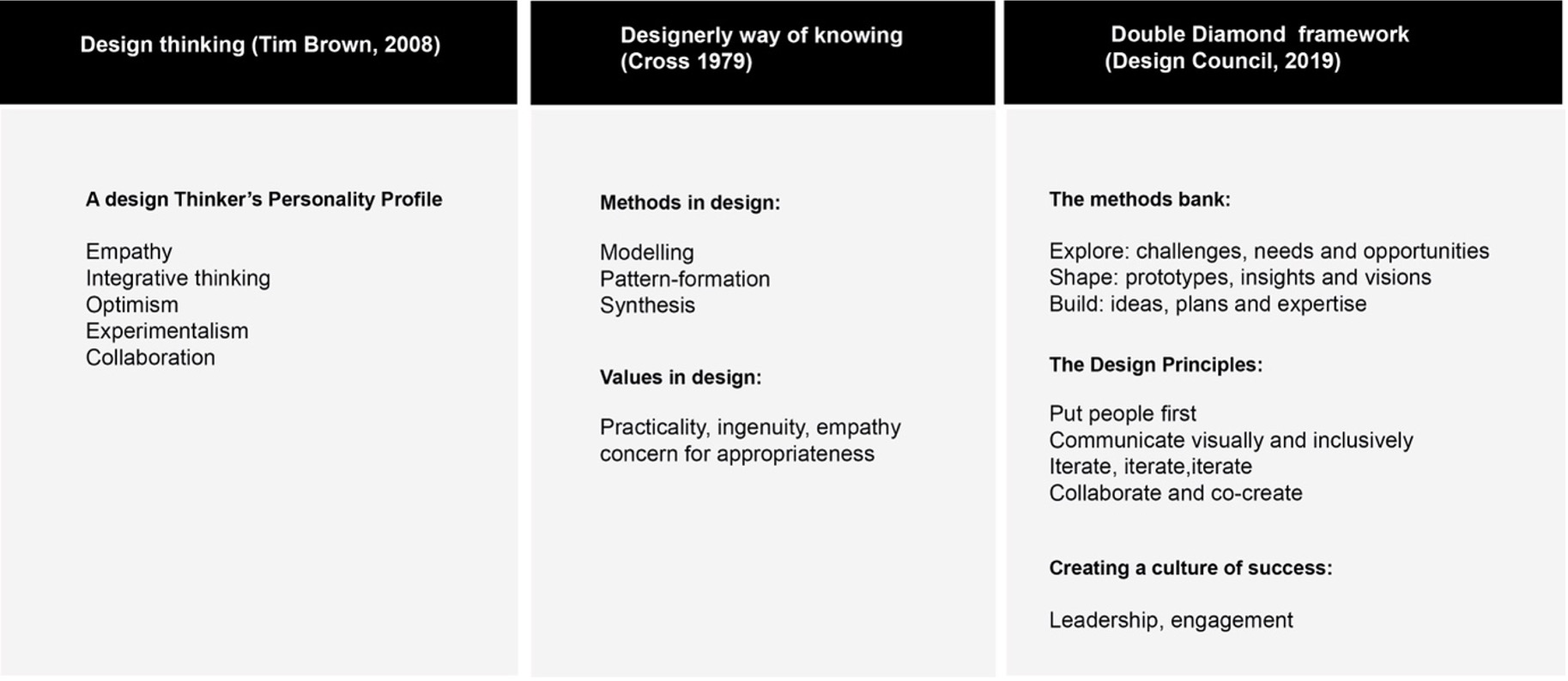
With a solid grasp of design thinking epistemology and processes, coupled with the adoption of a designerly approach to project guidance, design characteristics can function as enhancements that give rise to mindsets, methods, and principles. Figure 8 listed three examples, among these design principles, certain key elements emerge as particularly significant.
These three categories (Figure 6, Figure 7, and Figure 8) encompass what design thinking is—knowing (Figure 6), the design thinking process—thinking (Figure 7), and what specific methods are involved—doing (Figure 8)—across leading design theories and frameworks. This process of review provides a structure for the categorization of HPH design frameworks in the final stage.
4. Discussion
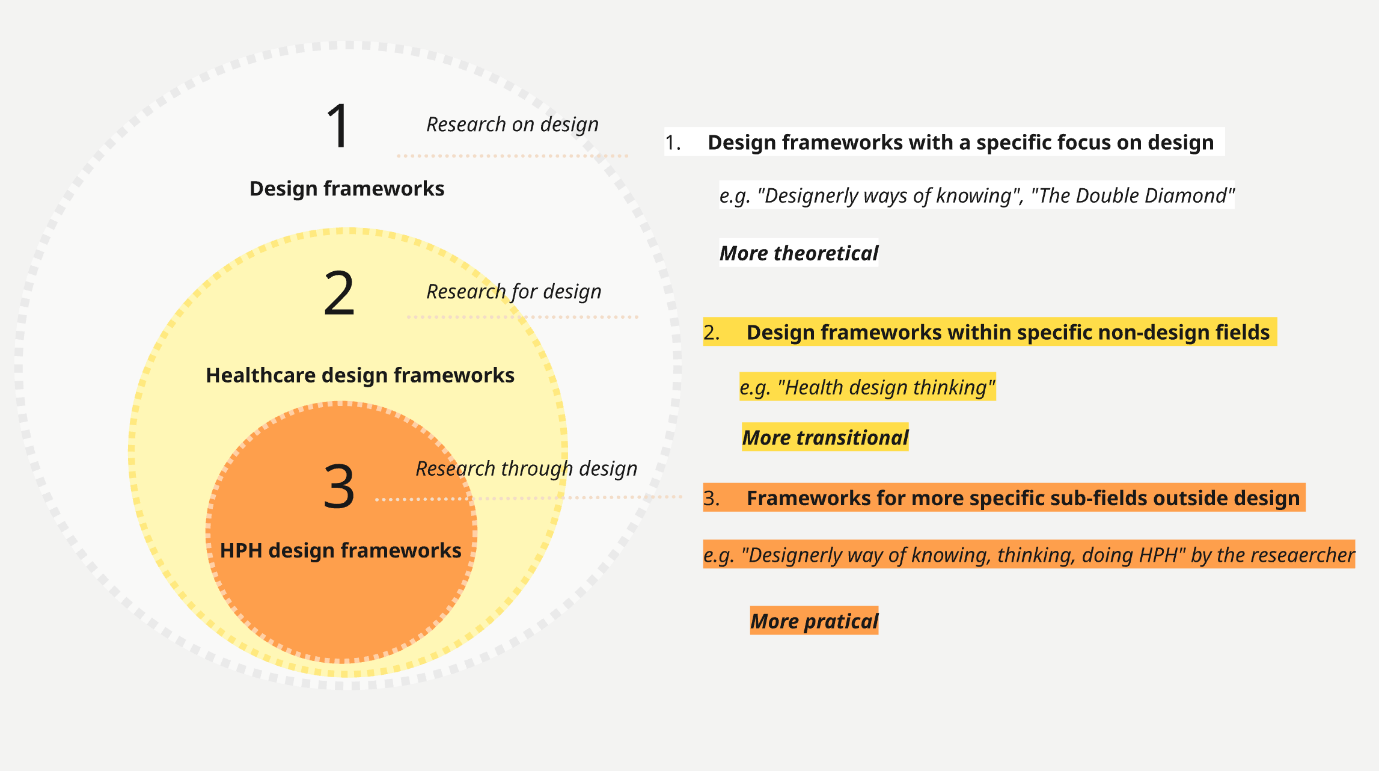
The response from Chinese HPH practitioners and leaders suggests these frameworks enhance understanding of the scope and methodology of design, developing and broadening the design thinking perspective within HPH. Future stages of the project will involve testing frameworks through further local initiatives. It is important to note that this paper does not attempt to prove the effectiveness of these frameworks. Instead, it sheds light on the rigorous research process behind their development, while also reflecting on the typology of design frameworks and the methods employed to create them. Different design frameworks can be divided into three types (Figure 13):
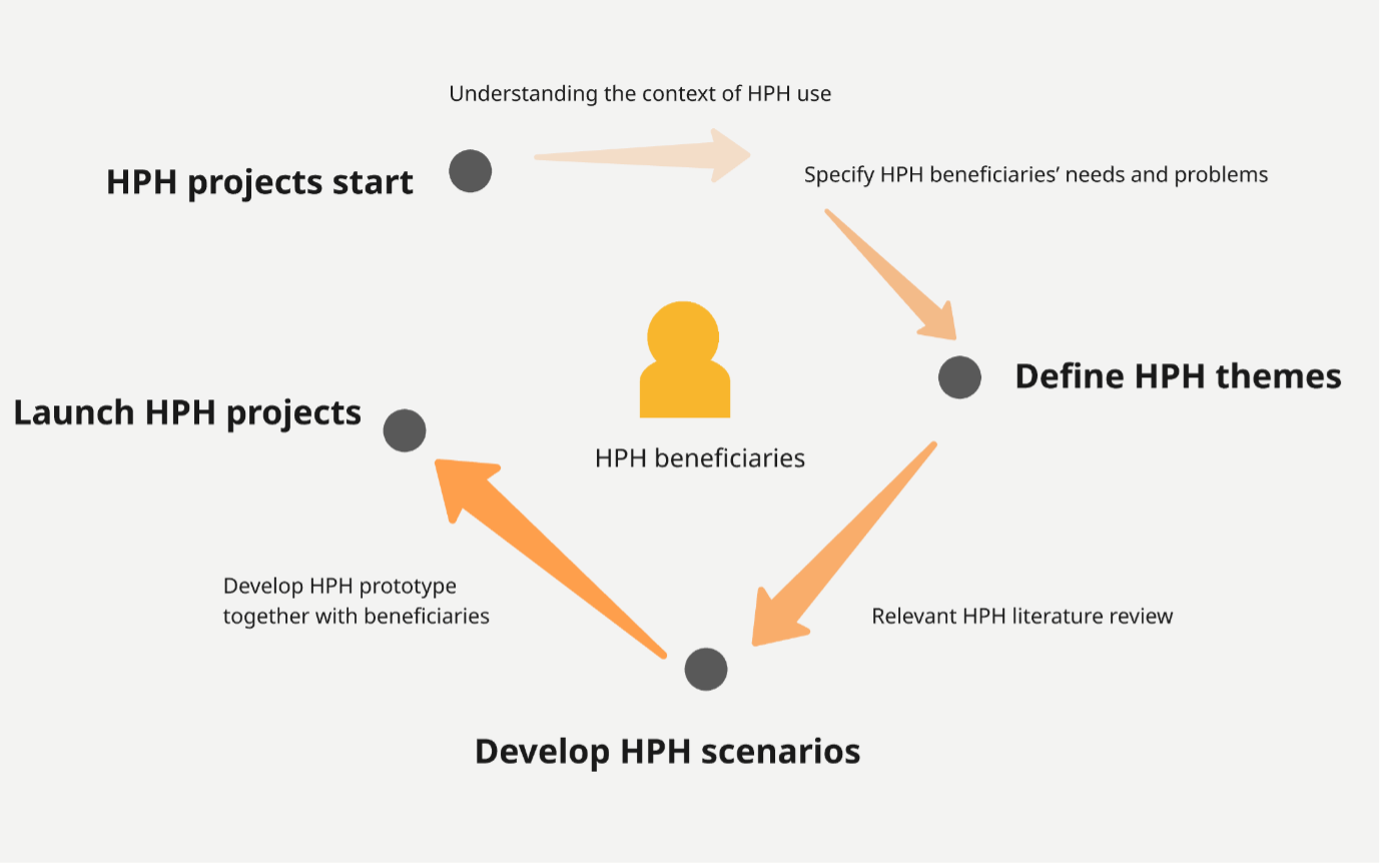
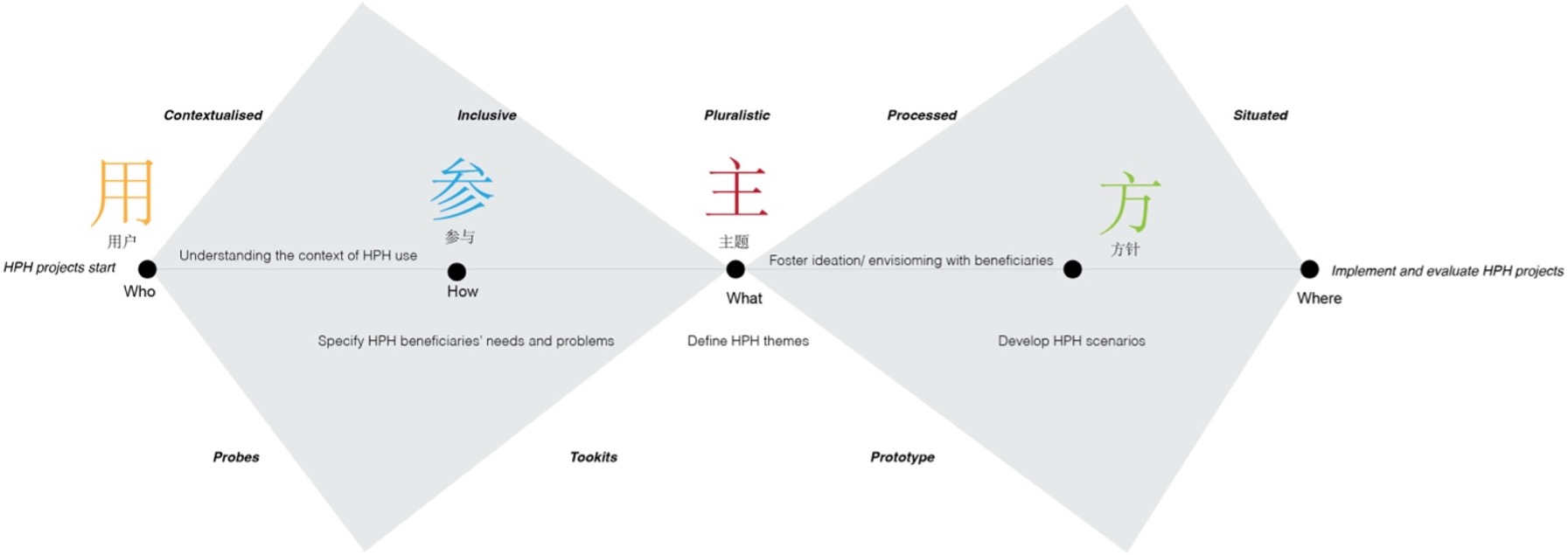
Based on the design thinking process review (Figure 7), the practice process map—a designerly way of doing HPH— (Figure 11) was generalized. When an HPH project starts, the first step is understanding the context of HPH use and specifying the focus group’s needs and problems, allowing them to define exactly what they should promote as the theme of the HPH project. The second step meant conducting relevant HPH literature and project reviews, then developing prototypes and scenarios together with beneficiaries to identify adaptive solutions or possible health promotion approaches. Finally, the HPH project could be launched and implemented into other similar contexts, communities, or focus groups.
4.1. Design Frameworks with a Specific Focus on Design
This framework is well-suited for research on design, emphasizing ontology and epistemology from an academic perspective. Figure 6 shows examples of these design frameworks, such as, The Double Diamond, the Danish Design Ladder, “designerly ways of knowing” from Cross and “Design thinking” from Brown. These frameworks examine design research and can be utilized by both designers and non-designers to gain a better understanding of design and its applications. Due to its broad scope and widespread use in both academic and non-academic domains, these frameworks have become generally popular.
Though these frameworks have universal applicability, fitting various domains, their broad scope can be a drawback as they may lack specific guidance in more specialized areas such as healthcare design, where more detailed navigation may be needed. Furthermore, when design studies are integrated into different non-design fields, both the design pathway and methodology can vary significantly from one discipline to another. It is therefore essential to explore and establish specific design frameworks tailored to individual disciplines.
4.2. Design Frameworks within Specific Non-Design Fields
The second category comprises design frameworks working within non-design disciplines not easily or immediately associated with design, such as healthcare. One design thinking framework for healthcare management and innovation lists “empathy, radical collaboration and rapid prototyping [38],” another design frameworks highlights health design thinking is “human centred (empathy, co-design and determinants) and creative mindset (questioning, visualizing, prototyping and storytelling) [39].”
The objective of this category of frameworks is “research for design,” aimed at informing and guiding the design process and nurturing design capability within specific interdisciplinary fields. Frameworks within this category must be contextualized where design is specifically applied. To develop an effective framework, designers and non-designers should collaborate and engage in mutual learning, acquiring a thorough understanding of the theories, methods, and practices of both fields before constructing a mature and symbiotic framework.
Despite this second design framework category focusing on how design thinking operates within specific domains—offering relevant understanding for non-design experts working in fields where design is being integrated—these frameworks may still be insufficient when it comes to addressing specific practices. For instance, a design framework for healthcare design may not be suitable for HPH, particularly regarding practical methodologies. This calls for a third category: design frameworks for sub-fields of each non-design domain.
4.3. Frameworks for More Specific Sub-Fields Outside Design
This category of frameworks fits into “research through design,” offering non-design experts an alternative—designerly approach to conducting research or practice through design methods. My set of design frameworks for HPH falls within this third category. These HPH frameworks offer more practical guidance in terms of methodologies, practice processes, and strategies.
Notably, it considers the current Chinese HPH approach and their existing design cognition, contextualising these elements to facilitate a shift in understanding from the present situation to a preferred state.
To develop this third level of specialized design frameworks—in addition to the collaboration and mutual learning emphasized in the second category—it is essential to incorporate action research and case studies. These methods help explore the practical dimensions of a framework’s use within specific contexts, ensuring that the resulting practical design is well-informed and grounded in real-world applications before it can be generalized to a broader context. Considering the dynamic nature of the contexts in which these frameworks are applied, design frameworks need to be flexible, flowing, semi-structured entities that can and should be continually updated based on changes in context, rather than maintaining a fixed, unchanging structure. The “Framework for Innovation,” as an evolved iteration of the “Double Diamond” framework, serves as an excellent illustration of how design frameworks can and should be adapted over time to better serve their purpose.
Overall, these three types of design frameworks serve different purposes in different situations. The first category of design frameworks is more theoretical due to its broad scope, used when people study design theories and methods. The second category, encompassing frameworks within the specific non-design fields, offers a mindset shift and different set of principles. It aims to equip non-designers with design knowledge, ultimately encouraging a transition from traditional perspectives within their fields to a new viewpoint. Lastly, the third category – composed of frameworks for sub-fields – provides more practical methodologies that enable non-design practitioners to conduct practice ideally without requiring the assistance of designers or design researchers.
The first category aligns with “research on design,” which can be seen as synonymous with “research into design” or “research about design,” as these frameworks primarily investigate the nature of the design field. The second type of framework pertains more to “research for design,” informing the design process within other specific interdisciplinary design fields, such as healthcare design. The third layer of frameworks relates more closely to “research through design,” using design as a way of knowing and doing within particular practices that underpin interdisciplinary design fields. “Designerly way of knowing, thinking and doing HPH” discussed in this paper suit in the third category.
2. Literature Review
2.1. Primary Literature Review
During the initial year of researcher’s PhD, he conducted an HPH primary literature review to understand better both background and research objectives, encompassing the HPH political and historical context, as well as its theoretical framework. This review included an examination of both global and Chinese contexts, drawing from sources such as WHO policy papers and academic literature.
The concept of HPH originates from the definition of health promotion (HP) “the process of enabling people to increase control over, and to improve their health [8].” Five key actions of HP were identified: “building public health policy; creating supportive environments for health; strengthening community action for health; developing personal skills; reorienting health services.” These actions have served as the primary political framework guiding national practices, including Chinese HPH [9].
Building on HP principles, HPH sees hospitals as active settings to promote health, encouraging a transformation in hospital roles from a treatment-centered approach to a dynamic, health promotion-focused approach. “A health promoting hospital not only delivers high-quality medical and nursing services but also fosters a corporate identity that upholds the goals of health promotion, cultivates a health-promoting organizational structure and culture with active, participatory roles for patients and staff, and develops a health-promoting physical environment while engaging in close cooperation with the community [10].”
The dominant framework identified is the 18 HPH core strategies and 7 implementation strategies [11]. This enfolds seven strategies for patients, staff, and the community, including “health promoting self-reproduction, health promoting co-production, empowering hospital setting for stakeholders, empowering illness management (health education) for stakeholders, empowering lifestyle development (health education) for stakeholders, health promotion and empowering community development for stakeholders [12].” Other well-known frameworks, such as PRECEDE-PROCEED [13] and RE-AIM [14], employ initials derived from key strategies, creating a secondary meaning as a method to develop a memorable and easily implementable framework.
Chinese HPH officially commenced in 2013. Following the ninth WHO Global Conference on HP in Shanghai in 2016 [15], during which the Shanghai Declaration on Promoting Health for 2030 [16] and the Agenda for Sustainable Development and the Healthy China 2030 [17] programmes were outlined. These government documents serve as a guide for hospitals to execute health promotion projects. However, when Chinese HPH literature discusses HPH theory, they primarily rely on political guidelines and practices based on WHO strategies and Western studies [18]. There is a lack of a theoretical framework grounded in the Chinese context [19].
The primary literature review contributed to a comprehensive understanding of the HPH content and theory, providing a robust background informing the action research conducted during the second and third years of researcher’s PhD. While these frameworks offer valuable theoretical guidelines and content, they do not delve into specific methods, particularly from a design perspective. Traditional frameworks based on the social sciences mentioned above often rely heavily on text-based descriptions, in contrast to the visual diagrams commonly used in design, which effectively convey logical thinking processes. To address this gap, action research was carried out—field trips and case studies—to gain insight into the field and ultimately to develop comprehensive design frameworks.
3.2. The Second Design Framework: A Designerly Way of Thinking for HPH
This framework serves as a reminder of the aspects overlooked by the current Chinese HPH approach. It illustrates that any design framework needs to consider the current cognitive orientations based on users’ contexts. If design is understood as “changing existing situations into preferred ones [36],” this framework methodology establishes a connection between the current approach and the preferred one. One of the purposes of delivering design frameworks is to help audiences – particularly those without a design background – to shift their mindset from an existing situation to a preferred one through means of visual design.
Based on the findings from my field trip and a subsequent comparative reflection on Chinese HPH practices, it was clear there were some weaknesses in their approach:
3.2.1. Who用户: HPH Beneficiaries
HPH beneficiaries – also the focus or target group – should be identified before any health promotion initiative. In Chinese HPH, where the approach tends to be standardized, it is crucial to establish a more targeted strategy recognizing different target groups. This process should consider contextual factors, including geographical and ethical uniquenesses.
3.2.2. How参与: Participation
Once a focus group has been identified, the next stage involves engaging and participating with it to understand individual needs and concerns regarding health promotion in daily lives. It is essential that the participation process is inclusive for all focus group members.
3.2.3. What主题: Theme
Once a focus group has been identified, the next stage involves engaging and participating with it to understand individual needs and concerns regarding health promotion in daily lives. It is essential that the participation process is inclusive for all focus group members.
3.2.4. Where方针: Orientation
Finally, hospitals can develop appropriate HPH implementation strategies and methodologies: these may also be interpreted as orientation, a systematic approach to align with identified health promotion themes and the special needs of a focus group.
Same as other exiting framework- RE-AIM [37], he strategy involves using the abbreviation (缩写) and the homophones (谐音) of Chinese characters to encapsulate the function of the framework. The “Who-How-What-Where” mnemonic is often employed as a starting point for basic project inspiration, while the Chinese abbreviation “用参主方” is derived from the characters 用户 (user), 参与 (participation), 主题 (theme), and 方针 (Orientation), connoting the main ingredients of a recipe. This can be further shortened to “参方.” From a traditional Chinese medicinal perspective, these characters represent the ingredients for a prescription, indicating paths for diagnosis. This method of identification renders the framework more memorable, user-friendly, and easily diffusible, a diagnostic tool that appropriates Chinese cultural and linguistic elements to help identify problems.
3.3. The Third Design Frameworks: A Designerly Way of Doing HPH
The most frequent health promotion approach found during the field trip is a top-down, linear process. When each department or organization implements health promotion projects, they choose a theme based on professional healthcare knowledge from within their faculty. For instance, the Centre for Disease Control and Prevention will promote methods of prevention of certain epidemic diseases, then design specific visual materials, either posting them on social media themselves or hiring designers to create media to display inside hospitals or local community premises. This process is still very much a traditional mass media communication approach, seeing end users as passive receivers of health knowledge. The staff from each department decides what to promote as well as where and how. In contrast, the researcher’s two case studies demonstrate a bottom-up strategy, where the health theme is defined after working together with local communities or focus groups.
Conclusion
While we acknowledge the value of frameworks in facilitating knowledge dissemination, there is a noticeable lack of discussion around the types of design frameworks and the methods of producing these frameworks. This paper aims to bridge this gap by demonstrating the rigorous research process behind the creation of design frameworks for Chinese HPH, involving a literature review, field trips, and case studies as action research. It serves as an exemplar for one ideal development of design frameworks, highlighting the importance of combining theoretical studies with action research. Additionally, the paper identifies three distinct types of design frameworks suitable for different scenarios, urging design researchers to consider factors carefully: for example, what types of design framework they would like to develop, who the target audiences of these frameworks may be, the purposes of dissemination, any current understanding or existing approaches to design thinking and practice, and potential gaps that the framework could address. Lastly, it emphasizes the need for effective communication strategies to ensure successful collaboration between designers and non-design professionals when utilizing these frameworks.
A transitional communication method was used in the process of this development, helping shift understanding from that contained hermetically within existing domains. One strategy using abbreviations and homophones to name the framework can result in a more creative, memorable, and easily disseminated. Moreover, it is crucial to emphasize that design frameworks must remain connected to real-world contexts. When applying these frameworks in practice, it is essential to continuously assess their relevance and fit within the specific context. This indicates that design frameworks should be viewed as dynamic structures subject to regular review and updating, rather than fixed and unchangeable constructs.
Email: mspl@michelangelo-scholar.com
Tel: +852-66761250
WHATSAPP:+60 11-2370 2845
Room A, 3/F, Wing Tat Commercial Building, 121–125 Wing Lok Street, Sheung Wan, Hong Kong, China
JDSSI
MSPL
JACAC
DH
JAUD